400-998-5282
专注多肽 服务科研
400-998-5282
专注多肽 服务科研
编号:635311
CAS号:
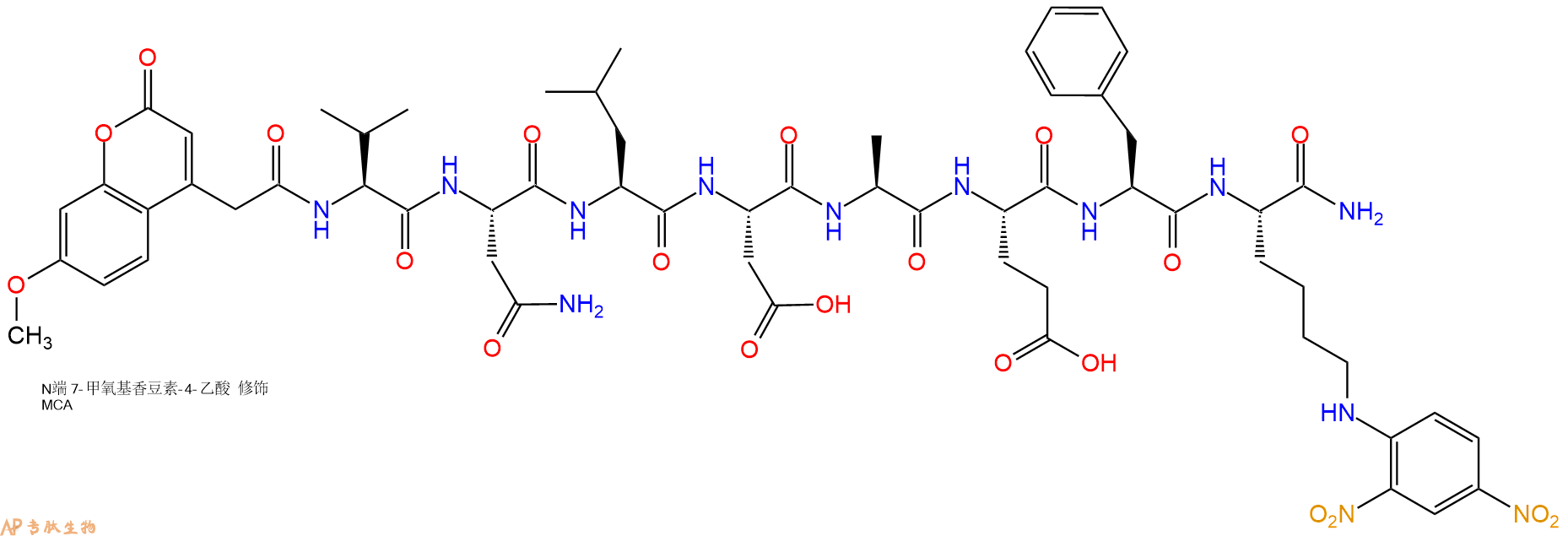
单字母:Mca-VNLDAEF-K(Dnp)-CONH2
荧光标记所依赖的化合物称为荧光物质。荧光物质是指具有共轭双键体系化学结构的化合物,受到紫外光或蓝紫光照射时,可激发成为激发态,当从激发态恢复基态时,发出荧光。荧光标记技术指利用荧光物质共价结合或物理吸附在所要研究分子的某个基团上,利用它的荧光特性来提供被研究对象的信息。荧光标记的无放射物污染,操作简便等优点,使得荧光标记物在许多研究领域的应用日趋广泛。人们利用利用荧光标记的多肽来检测目标蛋白的活性,并将其发展的高通量活性筛选方法应用于疾病治疗靶点蛋白的药物筛选和药物开发(例如,各种激酶、磷酸酶、肽酶等)。专肽生物经过长期开发,能够提供技术成熟的各种荧光标记多肽。
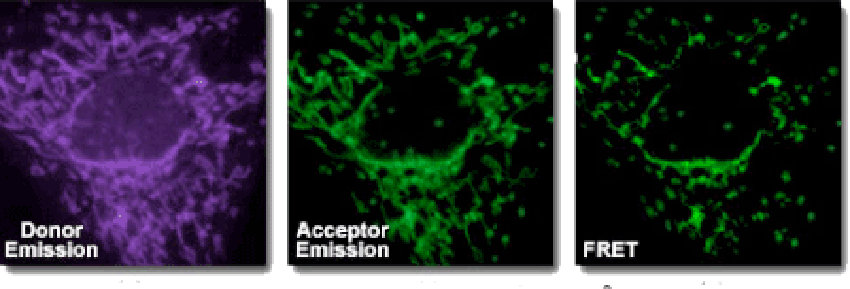
荧光共振能量转移(FRET)是一种非辐射能量跃迁,通过分子间的电偶极相互作用,将供体激发态能量转移到受体激发态的过程。此过程没有光子的参与,所以是非辐射的。该分析方法具有快速、敏感和简单等优点。
用于FRET试验的染料是可以相同的。但在大多数应用中其实是使用不同的染料。例如,一个供体基团(EDANS)和接受基因(DABCYL)匀被连接到一HIV蛋白酶的天然底物上,当该底物未被切断时,DABCYL可淬灭EDANS,从而检测不到荧光。当该底物被HIV-1蛋白酶切断后,EDANS不再被DABCYL淬灭,随即可检测到EDANS荧光。蛋白酶抑制剂的有效性可凭借EDANS荧光强度的变化进行监测。
FRET肽是研究肽酶特异性的便利工具,由于其反应过程可被连续监测,为酶活性的检测提供了一个便捷的方法。供体/受体对的肽键水解后产生的荧光可衡量纳摩尔级浓度的酶活性。当FRET肽是完整的,表现出的是内部的荧光猝灭,但当供体/受体对的任何肽键断裂就会释放出荧光,此荧光可被连续检测,从而可对酶的活性进行定量分析。FRET 肽可作为各类酶研究的合适底物,比如:肽酶、蛋白酶、激酶、磷酸酶的动力特征和功能特征;对新的蛋白水解酶的筛选和检测;对多肽折叠的构象研究等。
1、常用FRET的标准染料组合。
| 常用FRET的标准染料组合 |
| FAM/Lys(Dabcyl) |
| FAM/TAMRA |
| MCA/Lys(Dnp) |
| Abz/Tyr (NO2) |
| Abz/Dnp |
| Abz/EDDnp |
| Dabcyl/Glu(EDANS) |
| Dansyl//Glu(EDANS) |
2、FRET共振能量转移引发荧光猝灭的激发与发射波
| 猝灭剂 | 荧光团 | 激发波(nm) | 发射波(nm) |
| Dabcyl | Edans | 336 | 490 |
| Dansyl | Trp | 336 | 350 |
| DNP | Trp | 328 | 350 |
| DNP | MCA | 328 | 393 |
| DNP | Abz | 328 | 420 |
| Tyr (NO2) | Abz | 320 | 420 |
3、常规RET供体(Donor)-接受(Aceptor)对的福斯特临界距离(Forster Critical Distance)
| 供体 | 受体 | 福斯特临界距离(nm) |
| Cy5 | Cy5.5 | >8.0 |
| B-Phycoerythrin | Cy5.5 | 7.2 |
| FITC | Eosin Thiosemicarbazide | 6.1-6.4 |
| Rhodamine 6G | Malachite Green | 6.1-6.4 |
| BODIPY FL (1) | BODIPY FL (1) | 5.7 |
| GFP | YFP | 5.5-5.7 |
| Cy3 | Cy5.5 | 5 |
| Fluorescein | Tetramethylrhodamine | 4.9-5.5 |
| CF (2) | Texas Red | 5.1 |
| CFP | GFP | 4.7-4.9 |
| Dansyl | Octadecylrhodamine | 4.3 |
| Dansyl | FITC | 3.3-4.1 |
| BFP | DsRFP | 3.1-3.3 |
| IAEDANS (4) | DDPM (3) | 2.5-2.9 |
| Tryptophan | Dansyl | 2.1 |
| (1): 4,4-difluoro-4-bora-3a, 4a-diaza-s-indacene | ||
| (2): carboxyfluorescein succinimidyl ester | ||
| (3): N-(4-dimethylamino-3,5-dinitrophenyl) maleimide | ||
| (4): 5-(2-iodoacetylaminoethyl)aminonaphthalene-1-sulfonic acid | ||
对于分子生物学来讲,生物分析手段的发展,是阐明机理的必要条件。在研究分子间相互作用的道路上,人们不断探索,总结出很多方法,免疫技术,晶体衍射,核磁共振等。1948年,荧光共振能量转移(Fluorescence resonance energy transfer,FRET)理论被首次提出,它可以测定1.0-6.0nm距离内分子间的相互作用。1967年,这一理论得到了实验验证,将1.0-6.0nm的距离称为光学尺。二十世纪八十年代出,通过科学家的不断探索,Fret技术成功运用到蛋白质结构的研究中。自Fret荧光共振能量技术诞生以来,已结合多种先进的技术和方法,如电子显微镜,X射线衍射等,推动了分子生物学检测手段的发展。
荧光共振能量转移技术,是采用物理方法去检测分子间的相互作用的方法。他适用于在细胞正常的生理条件下,验证已知分子间是否存在相互作用。此方法的检测原理如下;
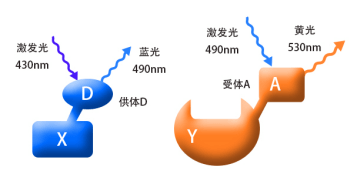
将我们要检测的蛋白(如图X和Y),分别偶联上D和A荧光蛋白,D和A是一对荧光物质,我们称之为供体(donor)和受体(acceptor)。当用430nm的紫光去激发X融合蛋白时,它能够产生490nm的蓝色荧光;同样,当我们用490nm的蓝光去激发Y融合蛋白时,它能够产生530nm的黄色荧光。(结合图1) 。
当蛋白X和Y间没有相互作用时(两者的空间距离>10nm),融合蛋白X和Y分别产生相应的荧光而被检测到,
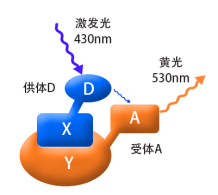
如果蛋白X和Y间存在相互作用(两者的空间距离需<10nm,结合图2),用紫光激发融合蛋白X其产生的蓝光会被融合蛋白Y吸收,从而产生黄色荧光,这时,在细胞内将检测不到蓝色荧光的存在。这时因为能量从X融合蛋白转移到了Y融合蛋白,这就是荧光共振能量转移技术。
一个理想的Fret相互作用体系,要求要有一对合适的荧光物质, 即供体的发射光谱与受体的吸收光谱有明显的重叠。且当供体的激发波长时对受体无影响,供体和受体的发射光谱要完全分开,否则容易造成光谱干涉,而使反应体系不稳定。目前,较为常用的供体-受体分子对,主要有绿色荧光蛋白类(GFPs)和染料类。绿色荧光蛋白类有CFP-YFP,BFP-GFP,BFP-YFP等,染料类的有Cy3-Cy5,FITC-Rhodamine等。且这些荧光物质要能够标记在研究对象上。
| 优点 | 缺点 |
| 在活细胞的正常生理条件下进行检测,观察大分子在细胞内的构象变化与相互作用,并弥补了需破碎细胞检测相互作用的缺点 | 应用比较局限,一般需要在待检测分子上偶联荧光物质(加上标记) |
| 灵敏度高,可实现对单细胞水平的研究,研究单个受体分子 | 对实验要求较高,如供受体的光谱重叠不好,会导致荧光干扰,对供受体的抗干扰能力,水溶性等要求高 |
| 可与多种仪器和技术结合使用,如显微镜,色谱技术,电泳,流失细胞技术等 | 需要不断探索合适的供体和受体,且能够标记分子 难以观察瞬时的分子间作用,检测要求大量的样品 |
以荧光物质CFP(供体)-YFP(受体)为例,检测AB蛋白在细胞内的相互作用。
最常见的一对标记组合是 Dancyl和Edans,

在本例中,荧光团 (EDANS) 和猝灭剂 (DABCYL) 与 HIV 蛋白酶的天然底物相连。在未裂解的底物中,DABCYL 淬灭 EDANS,因此没有可检测到的荧光。底物被 HIV-1 蛋白酶切割后,DABCYL 不再淬灭 EDANS,从而检测到 EDANS 荧光。然后可以监测 EDANS 荧光强度的变化以评估蛋白酶抑制剂的效率。

FRET 肽可用于研究肽酶特异性,因为它们可以连续监测反应,从而快速确定酶活性。供体/受体对之间的肽键可以被切割,从而产生荧光信号以测量纳摩尔浓度的酶活性。当未被切割时,FRET 肽会淬灭内部荧光;然而,供体/受体对之间肽键的断裂会释放出可以连续检测到的荧光信号,从而可以量化酶的活性。
FRET 肽在许多不同的酶研究中用作合适的底物:
肽酶、蛋白酶、激酶和磷酸酶的动力学和功能表征。
筛选和检测新型蛋白水解酶。
肽折叠的构象研究。

Extracellular amyloid-β peptide deposition into cerebellar plaques and formation of intracellular neurofibrillary fibers accompanied by the loss of neurons are characteristic histopathological lesions found in the brains of Alzheimer‘s disease patients. Individuals suffering from this disease show a gradual loss of cognitive functions and disturbances in behavior. Apart from some rare familial forms of the disease, the onset of Alzheimer‘s disease is usually above 60 years. Since the risk to develop the disease increases with age, Alzheimer‘s disease has turned into a major health and social problem in “first world” countries with an increasing proportion of older people, and is going to become one in emerging states. In this brochure we present amyloid peptides and related products for Alzheimer‘s disease research.
ALZHEIMER’S DISEASE
Alzheimer‘s disease (AD) is the prevalent cause of dementia in elderly people and has become one of the leading causes of death in developed countries together with cardiovascular disorders, cancer, and stroke. It is estimated that more than 46 millions of people suffer from AD all over the world. As age advances, the risk for developing AD increases. The frequency of AD at the age of 60-64 is about 1% and doubles approximately every five years. By the age of 90 and older, approximately 50% of the population suffers from this disease. AD is an irreversible and progressive neurodegenerative disorder. Symptoms include gradual loss of cognitive functions such as memory, verbal and visuospatial abilities, changes in personality, behavior, and activities of daily living. AD patients in the final stages are completely dependent on the care of others.
The characteristic lesions in the brains of AD patients were first described by the German neuropsychiatrist Alois Alzheimer in 1906 during the post-mortem examination of a mentally ill patient whose deterioration he had observed until her death. The lesions consisted of dense extracellular deposits, now designated as neuritic or senile plaques, and intracellular dense bundles of fibrils, which are now known as neurofibrillary tangles.
Currently, diagnosis of AD with adequate testing is approximately 90% accurate. It is based on the exclusion of a variety of diseases causing similar symptoms and a careful neurological and psychiatric examination, as well as neuropsychological testing. Imaging technologies for detecting amyloid plaques and tangles in vivo are becoming more precise and thus a valuable additional tool. Numerous potential biomarkers as α1 -antitrypsin, complement factor H, α2 -macroglobulin, apolipoprotein J, and apolipoprotein A-I for diagnosing AD are being evaluated. However, post-mortem histopathological examination of the brain is still the only definite diagnosis of this disease.
AD can be either inherited or sporadic. The inherited or familial AD is rare and comprises only 5-10% of all cases. Autosomal dominant mutations in the amyloid β/A4 protein precursor (APP) gene on chromosome 21 and the presenilin-1 or -2 genes on chromosomes 14 and 1, respectively, have been attributed to the early onset (before the age of 65) of this disease.
APP belongs to the type-1 integral membrane glycoproteins with at least 10 isoforms generated by alternative splicing of the 19 exons. The predominant transcripts are APP695, APP751, and APP770. A number of mutations within the APP gene have been detected in families with an inherited risk for early onset of AD. Usually, they are named after the region, in which they have been detected, e.g. the London APP717 mutations (V717I, V717F, V717G), the Swedish APP670/671 double mutation (K670N/M671L), the Flemish APP692 mutation (A692G), or the Dutch APP693 mutation (E693Q). The Swedish mutation of the β-secretase cleavage site of APP and mutations of positions 692-694 (Aβ 21-23), which strongly influence the aggregation behavior of Aβ, have been studied intensively.
A choice of relevant mutations in the Aβ region of APP is assembled in the table below.
| Exchanged Position in APP | Exchanged Position in Aβ | Designation |
|---|---|---|
| A673T | A2T | Icelandic |
| H677R | H6R | English |
| D678H | D7H | Taiwanese |
| D678N | D7N | Tottori |
| A692G | A21G | Flemish |
| E693D | E22∆ | Osaka |
| E693G | E22G | Arctic |
| E693Q | E22Q | Dutch |
| E693K | E22K | Italian |
| D694N | D23N | Iowa |
| L705V | L34V | Piedmont |
The presenilins are another group of proteins involved in the development of AD. Presenilins are integral membrane proteins with eight transmembrane domains localized in the endoplasmic reticulum and the Golgi apparatus. A multitude of mutations within the presenilin-1 and two within the presenilin-2 gene account for most of the cases of early onset of AD.
Genetic factors may contribute as well to the late onset of AD. Increased susceptibility is associated with the expression of different apolipoprotein E (ApoE) isoforms due to the polymorphism in the APOE gene on chromosome 19. In the central nervous system, ApoE has been implicated in growth and repair during development or after injury. Carriers of the APOEε4 allele show a higher risk in developing the disease than carriers of the other two possible alleles APOEε2 and APOEε3. The ApoEε4 effect seems to be dose-dependent since individuals with two of these alleles seem to be at two-fold higher risk to develop the disease than those with one allele. Polymorphisms of the α2 -macroglobulin gene on chromosome 12 and the gene coding low-density lipoprotein receptor-related protein 1 (LRP1), LRP1-C/T, have also been suggested to be a risk factor for the late onset of AD. However, further studies in this field are required.
A number of additional, most diverse risk factors have been proposed. These include gender, ethnic group, head trauma, cardiovascular diseases, and educational level.
AD THERAPEUTIC STRATEGIES RELY ON DETAILED KNOWLEDGE OF THE MOLECULES INVOLVED
Women, Hispanics, individuals who have experienced a head trauma earlier in life, and persons who suffer from cardiovascular diseases appear to have a higher risk of developing the disease.
The etiology of AD is still not completely understood. Initial research focused upon determining the molecular structure of the senile plaques and the neurofibrillary tangles originally described by Alois Alzheimer. The main constituents of the senile plaques were identified as cleavage products of APP, designated as amyloid β-peptides (Aβ peptides).
Depending on the composition and the fraction of fibrillar to non-fibrillar forms of these amyloid peptides, several kinds of senile plaques can be distinguished. Three types of proteases, α-secretase, β-secretase (or β-site APP-cleaving enzyme, BACE), and γ-secretase are involved in APP processing. APP can either be processed by the α- and γ- or by the β- and γ-secretases. The major two amyloid peptides identified in senile plaques, amyloid β-protein (1-40) (Aβ40) and amyloid β-protein (1-42) (Aβ42), are generated by successive proteolysis of APP by β- and γ-secretases. Cleavage of APP by β-secretase results in the release of the extracellular N-terminal protein fragment known as soluble APP-β molecule (sAPP-β). Then, the membrane-retained APP is further processed within the transmembrane domain by γ-secretase to yield either Aβ40 or Aβ42. The formation of Aβ40 and Aβ42 is a normal process, and both peptides can be detected in the plasma and cerebrospinal fluid (CSF) of healthy subjects.
In most studies, similar concentrations of Aβ40 have been measured in the CSF of both healthy controls and AD patients. On the other hand, Aβ42 concentrations in the CSF of AD patients are significantly lower than in normal controls, probably reflecting an increased deposition as insoluble plaques.
The neurofibrillary tangles found inside neurons of Alzheimer’s brains are composed of paired helical filaments whose main components are hyperphosphorylated forms of tau, a microtubule associated protein involved in promoting microtubule assembly and stabilization. Self-assembly into paired helical filaments is believed to be a result of hyperphosphorylation due to either the increased activity of protein kinases or the decreased activity of phosphatases.
Several lines of evidence support the view that the accumulation of Aβ42 in the brain is a primary event in the development of AD. Increased cerebral Aβ production appears to be characteristic for all the mutations within the APP and the presenilin genes of familial AD. In patients with Down syndrome (trisomy 21), elevated levels of APP and Aβ due to a third copy of the APP gene result in deposition of Aβ at an early age between 20 and 30.
Formation of neurofibrillary tangles is considered as a consequence of Aβ deposition with a further impact on the progression of the disease possibly due to disruption of axonal transport mechanisms in neurons.
The detailed knowledge about the molecules involved in AD has led to the development of several therapeutic strategies.

One strategy aims at the reduction of Aβ40 and Aβ42 by inhibition of either β- or γ-secretase activity or by clearance of Aβ in the brain by means of immunization with these peptides. Transition metals as Cu, Fe and Zn play an important role in the pathology of AD. Aggregation and neurotoxicity of Aβ are dependent on the presence of copper, so Cu-chelating agents showed promising effects in animal models. Another approach is the prevention of the cellular inflammatory response in the cerebral cortex elicited by the progressive accumulation of Aβ. Further preventive therapeutic strategies are based on the findings that cholesterol-lowering drugs such as statins and estrogen replacement therapy reduce the risk of developing AD. An additional treatment alternative would be the inhibition of the serine-threonine protein kinases, glycogen synthase kinase 3 (GSK3) and cyclin-dependent kinase 5 (CDK5), which are probably responsible for the phosphorylation of the tau protein. Inhibition of calpain, an enzyme showing increased activity in AD brains, led to promising results in animal studies. Calpain cleaves the CDK5 activator p35 leading to p25 formation and CDK5 overactivation.
Several acetylcholinesterase inhibitors such as tacrine, donepezil, rivastigmine, and galantamine have been approved for the treatment of mild to moderate AD by the FDA and other authorities. They act by reducing the deficits of the neurotransmitter acetylcholine associated with cognitive impairment in AD patients. The amantadine derivative memantine, an NMDA receptor antagonist, which was already used for the treatment of moderate to severe AD in Europe, has gained approval in the United States by the FDA as well.
A promising drug candidate, the β-secretase inhibitor verubecestat (MK-8931) developed for the management of mild to moderate AD, has moved to phase III. Moreover, the BACE inhibitor AZD3293 showed encouraging results in clinical studies. Antibodies as aducanumab and solanezumab, which have been designed to degrade plaques and lower the level of Aβ in the brain, have reached advanced stages of clinical testing for mild cases of AD.
Despite the many promising therapeutic approaches, AD still remains a major burden for the patients, their relatives, and the society.
MCA标记肽的说明
(7-Methoxycoumarin-4-yl)acetyl is fluorophor with an excitation at 325 nm ▉ and emission of 392 nm ▉.
MCA标记肽相关文献:
Characterization of the Altai Maral Chymosin Gene, Production of a Chymosin Recombinant Analog in the Prokaryotic Expression System, and Analysis of Its Several Biochemical Properties.
Belenkaya, S. V., A. A. Bondar, T. A. Kurgina, V. V. Elchaninov, A. Yu Bakulina, E. A. Rukhlova, O. I. Lavrik, A. A. Ilyichev, and D. N. Shcherbakov. Biochemistry (Moscow), 2020.
IL-1b is an innate immune sensor of microbial proteolysis.
LaRock, Christopher N., et al. Science Immunology 100.200: 300 (2016).